-1.jpg)
LotusLink Co., Ltd. participates in “April Dream,” a project that turns April 1st into a day for sharing dreams. This press release outlines the dream of LotusLink.
Traveling Plagues
— LotusLink’s Challenge: Transforming Healthcare from Emerging Markets —
Today, April 1st, we speak of a dream we are determined to realize. This story begins with the harsh “reality” a single physician witnessed in a developing country—a reality far removed from what many consider normal. Knowing a world unknown to you, especially when that world is failing, becomes the catalyst to ask: “Is there something I can do?”
My life as a doctor was privileged from the start. After completing residency at my choice of hospitals in the U.S. and Japan, I spent over 20 years in cancer care at a central Tokyo hospital. I took pride in being Japanese, thinking, “The National Health Insurance system is wonderful!” while witnessing U.S. healthcare where insurance coverage often dictates treatment plans.
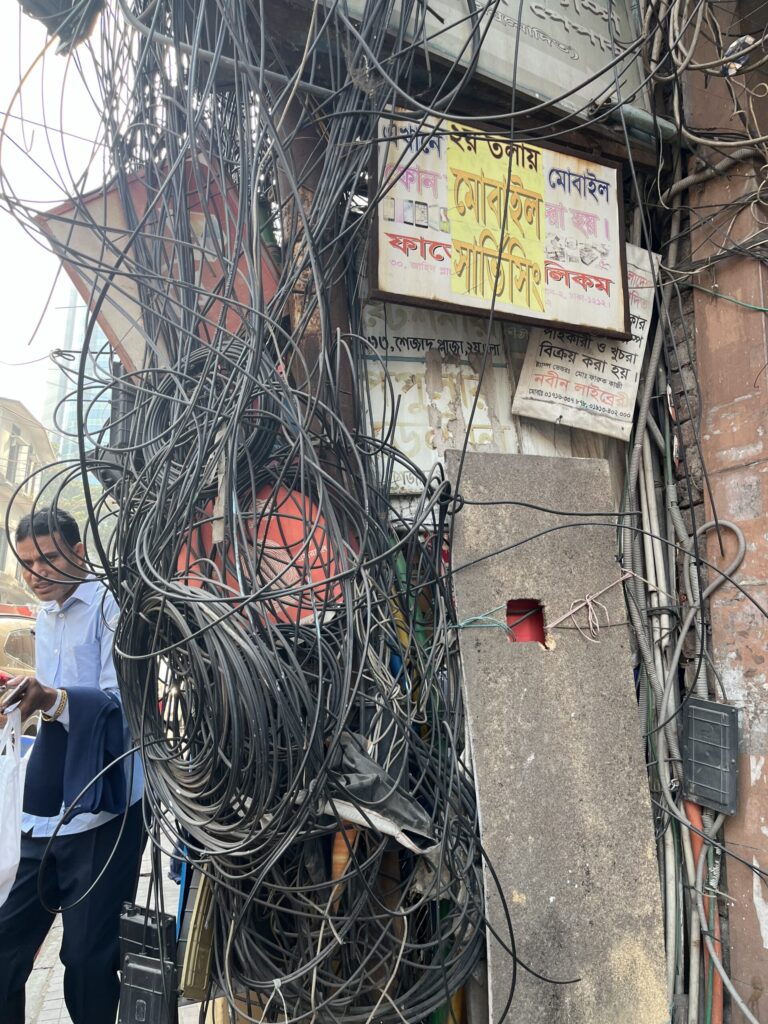
However, three years in South Asia, which forced themselves into my life, made me realize that my previous life had been a world protected by a series of miracles.
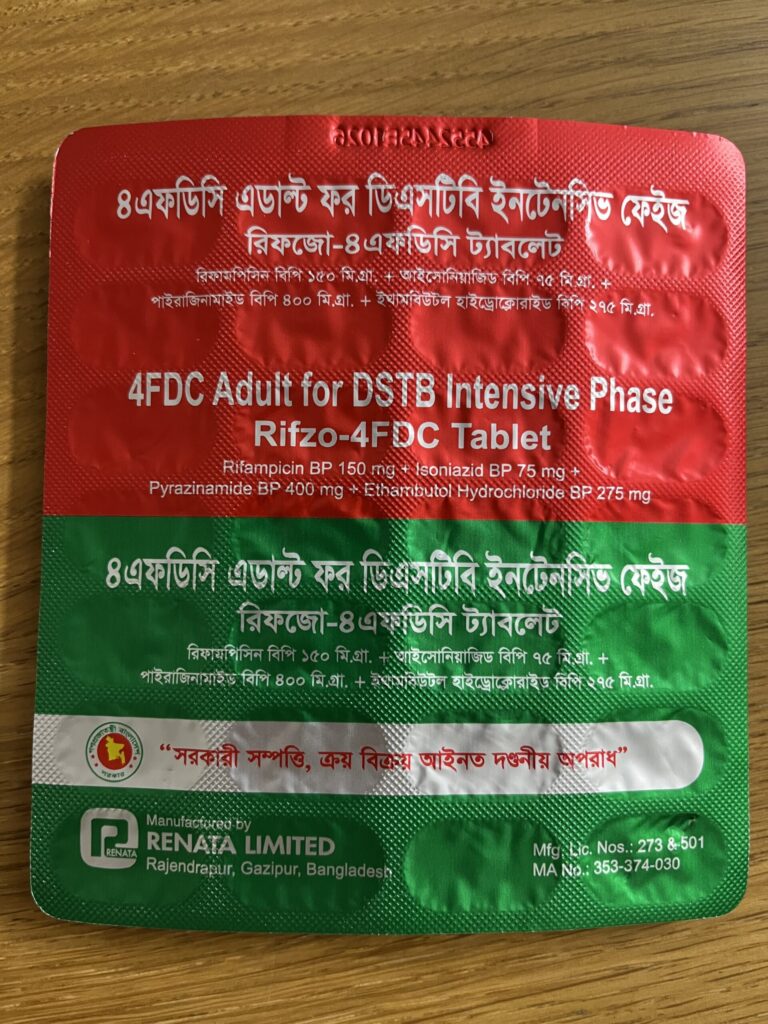
In that country, the poor cannot afford to visit a hospital when they get sickness. Instead, they can buy almost any medicine at a drugstore—no prescription required. The lineup is vast, ranging from antibiotics to anti-cancer drugs. Experienced drugstore clerks listen to customers’ symptoms and decide on the medication, despite having neither a medical nor a pharmacist license. Acetaminophen (fever reducer) costs about 2 yen per tablet, and Amoxicillin (antibiotic) is available for about 3 yen.
Conversely, those with wealth visit general hospitals when unwell. Since health insurance does not exist, a single visit often costs over 10,000 yen. It is a “lawless zone” of healthcare—at least, by the standards of advanced nations.


When Systems Fail, “Justice” Is Redefined
But was it only healthcare that was lawless in that country? Humans are social creatures; this is a human trait regardless of a nation’s wealth. Every country has laws, police, and judges. Yet, if judges accept bribes and police move based on personal feelings and tips, communal living cannot survive. People who have painfully learned that they cannot rely on the “systems” they should be able to trust develop unexpected behavioral patterns when facing hardship.
In a society where systems do not function, people begin to create their own “private laws” within family units. If a family member becomes successful, every relative—down to the most distant—demands support. Responding to these demands becomes “justice,” even if the request is ethically wrong or illegal. What the successful person says is absolute; if he extends a helping hand, he is a hero in the family community. Even if an act is illegal, if the law itself is non-functional, it can be justified through any excuse. In a country where “honor killings” are justified, the definition of “illegal” differs vastly from ours.

This successful figure is often called a “Banyan tree.” In South Asia, where patriarchal systems are still deeply respected, this is almost always the father. This social structure is reflected directly in healtcare. Where social systems have collapsed, healthcare also becomes uncontrollable.
People in that country often said of a person’s life: “You start thinking about death in your late 30s, become unable to work due to illness in your 40s, and die in your 50s.” Except for the urban wealthy, this is likely the cruel “normal” for those in rural areas, who make up the majority of the population. When illness or injury strikes, people give up easily because they have no options. This applies not only to patients but to doctors as well.
A Threat Without Borders
As a result, death is very close. Not just in healthcare, but in daily food, water, electricity, transportation, and education… the “Give Up” command appears early in every scenario. Meanwhile, the wealthy in developing nations possess riches they could not exhaust in a hundred lifetimes. Imagine how the world would change if even a fraction of that flowed into a system for the general public. In reality, internal political structures are complex, and it is not a problem easily solved. Often, the wealthy do not even share the value that “all humans are equal.”



Developing nations account for 74% of the world, and Official Development Assistance (ODA) from advanced nations and NGOs/NPOs are everywhere. If aid solved social problems, why are these countries still “developing” after decades? In lands with long colonial histories, surviving on aid from someone “upstream” has become part of the social fabric. The premise of standing up on one’s own may not even exist.
Is this just a story of a “distant country that has nothing to do with me”? What if you developed pneumonia one day and not a single antibiotic worked? The unbelievable stories from developing nations are not someone else’s problem. Antibiotics are sold without prescriptions and treatment is stopped halfway. The drug-resistant bacteria born from the inappropriate use of antibiotics spread across borders. As long as people move, diseases have no borders. When people travel from developing nations where resistant bacteria are rampant, those bacteria become unintentional “chemical weapons” scattered across the globe.
Filling the Healthcare Void with Data
With wars occurring worldwide, the balance of global wealth is shifting. No matter how strictly advanced nations follow treatment guidelines, those efforts can easily be undermined on a global scale as people migrate. So, what should we do?
LotusLink was founded with colleagues who share this sense of urgency. What I saw in South Asia was “Healthcare where data does not exist.” No one knows where which diseases are distributed. No one knows where the patients are. No one knows which treatments are effective.
That is why LotusLink wants to start by “making things visible.” We aim to travel through regions with mobile check-up vans, collect data, and visualize disease distribution and drug-resistant bacteria. We will then share that data with medical institutions and researchers.
Healthcare only progresses when there is data. Yet, even in 2026, most areas of our planet still have no data. 74% of the world consists of developing nations. If we can begin to visualize the state of healthcare through data, the world will surely change.
We must shift from the idea of “Saving someone else’s house (a poor country)” to the perspective of “Repairing the malfunctions in our shared home.”
Healthcare, Data, and International Business. We at LotusLink hope to one day work with those who resonate with this vision.
